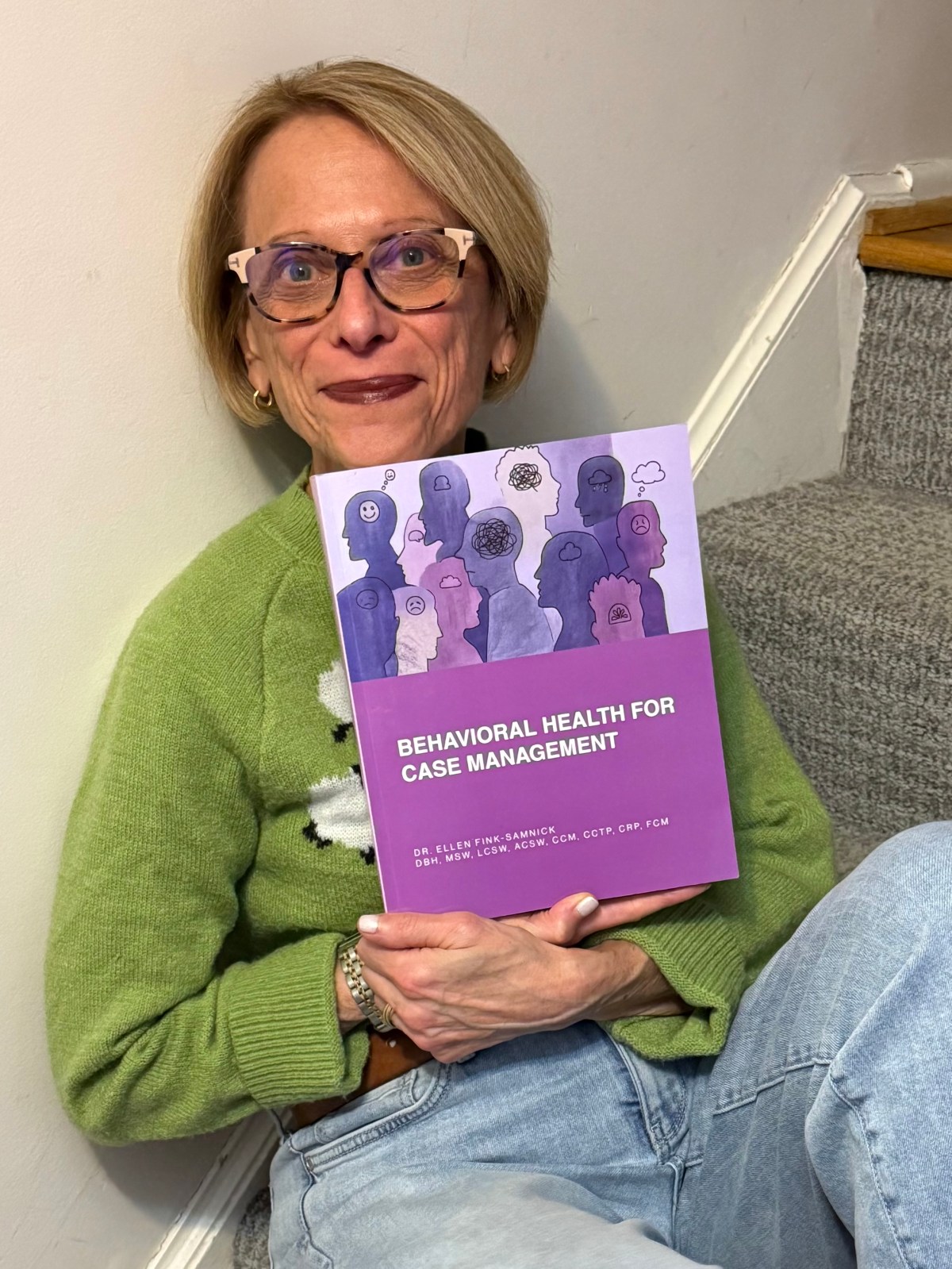
Over this past week I have been shouting from the rooftops that my latest, and 6th book is finally out! However, there is nothing like the intense emotion and sense of pride experienced by an author when they get to finally hold and see their finished product! Behavioral Health for Case Management published by Blue Bayou Press is out and now available for all to experience. Many have asked why I chose to focus on this topic for the book.
My intent has been part of a long-standing vision. For some time I wanted to craft a text for my interprofessional colleagues in case management that provided a practical view of the behavioral health issues experienced by patients, their families, and support systems. Too often I heard that they were forced to deal with these issues, though with limited knowledge, education or training on their real impact to practice.
I wanted to share some of the clinical knowledge taught to my social work and other behavioral health colleagues on psychopathology, human behavior across the life span, short-term interventions and treatment, assessment, suicidality, trauma, with the pillars of quality measures, regulations, and other key intel. Too often I was asked how my colleagues in nursing and other non-behavioral health disciplines could have access to my braintrust of this information.
I strived to provide guidance on screening and other innovative interviewing tools to best guide the issues and realities faced by my colleagues across practice settings and populations. There was little practical guidance in one place on the management of mental health realities for the LGBTQIA+ population; Military members, their families, and veterans; persons with visible and invisible disabilities; as well as women. Too often I received consults from my colleagues on where this information lived, and for their own use.
I wanted to create a unique Case Management Behavioral Health Conversation Map to guide interviewing and interventions with patients their families, and teams.Too often I was asked for a roadmap to guide interactions and dialgoues with patients who live with behavioral health and mental illness, as well as the key phases for case managers engaging with teams that coordinate care.
I hoped to advance current evidence-based intel on the manifestation of behavioral health’s impact on physical health, integrated care, and attainment of whole-person health. Too often I was sought out for data and research on population-focused information specific to diagnostic presentation and implications.
I dreamed of forging foundational knowledge through an authoritative text to level-set all students entering case management through the academic gateways of counseling, medicine, nursing, pharmacy, public health, social work, rehabilitation, and other interprofessional education programs. Too often my colleagues in academia asked me to write content that spoke to this mandate for the industry’s newest clinicians..
I imagined crafting an affordable book for onboarding and credentialing preparation of the case management workforce with practical application through case examples, original boxes, tables, and figures, and a robust index to guide individual learning. Too often I considered dialogues with case management thought-leaders who believed that this content should be required for credentialed case managers.
No single book or resource can do it all but hopefully I have attained my expectations and met yours as well.
Enjoy the learning! I look forward to hearing everyone’s perspectives.
Behavioral Health for Case Management is available on Amazon https://a.co/d/7anBopw
New Book on Behavioral Health for Case Management Provides Essential Workforce Knowledge
If you work in case management today, you must deal with behavioral health. My interprofessional colleagues have asked me for decades to write a book on the common behavioral health conditions experienced by patients, their families, and support systems. Too often it was shared with me that nurses and other non-behavioral health professionals in case management roles were forced to deal with these issues, though with limited knowledge, education or training on their real impact to practice. My newest book mitigates this gap in education and training.