

There is an industry priority to right the societal wrongs associated with historical trauma and systematic racism. These long-standing realities are key drivers of wholistic health disparities: physical, behavioral, and psychosocial health.. A fluid stream of outcomes mandate concordant approaches to racial, ethnic, and other cultural contexts of treatment (e.g., disability, familial choice, gender orientation, regional influences). Yet, despite research to validate data wholistic health outcomes, reflective quality metrics have not been developed.
What Are We Talking About?
Abundant data assesses the impact of historical, racial, and other types of trauma on health and behavioral health outcomes. Increased healthcare utilization has been identified for survivors of physical and sexual trauma, primarily minority women. Campbell et al. (2002) studied 2,355 females, 21-25 years old, enrolled in a large health maintenance organization (HMO). Patients who experienced intimate partner violence had a far higher prevalence (>50%-70%) of gynecological and central nervous system complaints (e.g., back and pelvic pain, fainting, headaches, seizures), plus other stress-related health issues (e.g., hypertension, insomnia, susceptibility to viral/bacterial infections). Purkey et al. (2020)identified trauma survivors as frequent users of primary, urgent, and emergency care for acute and chronic symptoms. Clarke et al., (2019) discussed the presence of vague somatic complaints by patients who endured traumatic experiences (e.g., ACEs, bulling, pressures to excel in school and career). Costly emergency department visits and ambulatory diagnostic tests are frequently used to identify etiology for chronic and diffuse pain, digestive problems, headaches accompanied chronic illness exacerbation, yet to no avail.
Another vital dyad for attention involves chronic pain management and stigma experienced by patients from marginalized communities. Wallace et al. (2021) completed a recent study; participants were trauma survivors (e.g., historical, racial, sexual) and members of indigenous, LGBTQIA+, or refugee communities. The results were telling. When physical and emotional pain were expressed to providers, they was minimized or dismissed. If acknowledged by providers, short-term prescriptions were given versus referrals to behavioral health and other specialists.
What Does it Imply?
Data mandates the need for intentional, sustainable quality improvement in this arena. Will the next generation of metrics account for this reality? Racism remains a major factor to drive racial and ethnic inequities in health and mental health, though fails to be addressed in healthcare’s quality proposition. Of the articles reviewed for this blog post, trauma-informed quality analysis of care remained elusive. 2021 saw a fresh generation of industry health equity measures, yet few addressed integrated care, let alone assesses wholistic health equity. Existing metrics continue to silo health or behavioral health. Insufficient focus has been on industry-vetted quality models addressing population-focused, concordant, trauma and equity-focused interventions.
Where Will Health Equity’s Quality Compass Point?
This author is developing a Quintile Aim for consideration, which adds the pivotal domain of Wholistic Health Equity to the industry’s seminal quality compass. NCQA continues to push this agenda in evolving new metrics. Public comment is open (until 3/11/22) for new HEDIS measures targeting the SDoH. Wyatt et al. (2016) posed a 5-step quality model for organizations to advance health equity delivery to the communities they served, addressed in Figure 1.
Figure 1: A Framework for Healthcare Organizations to Achieve Health Equity (Wyatt et al., 2016)

The model was well-intended though had limited substance or strategic action to leverage the intent. This effort was reminiscent of the Quadruple Aim; little data drove the model and obstructed full industry acceptance. By contrast, Dover and Belon’s (2019) Health Equity Measurement Framework (HEMF) is worthy of exploration. Based on the World Health Organization’s Social Determinants of Health model, HEMF vast evaluation areas to measure health equity at macro, meso, and micro levels, as shown in Figure 2.
Figure 2: HEMF Framework Elements (Dover & Belon, 2019)
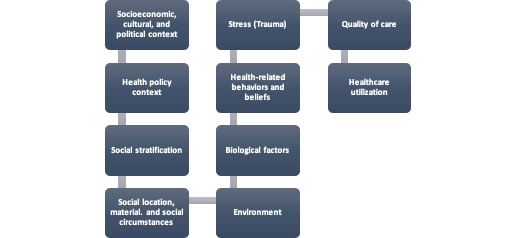
The HEMF model is worthy of a test drive to gauge its true merit. Use of the wide-scope of theoretical and evidence-based industry elements is an asset. Population diversity and complexity are accounted for through power-related and disparity measures. Health beliefs, behaviors, and values are acknowledged with stress factored in; the traumatic-response across circumstances is embedded. My desire to keep this post brief limits further elaboration on the HEMF model. However, know it poses strong value as a robust quality model to address health, behavioral, and racial health disparities across populations exposed to trauma’s diverse lens.
Have other integrated care quality models that account for wholistic health equity? Add your considerations and comments below!

Important information…thanks Ellen!
Get Outlook for iOS
________________________________
LikeLike
Since so much of our lifelong health comes from our childhood experiences, childhood mental health-care should generate as much societal concern and government funding as does physical health, even though psychological illness/dysfunction typically is not immediately visually observable.
The health of all children needs to be of real importance to us all, regardless of how well our own developing children are doing. A physically and mentally sound future should be every child’s fundamental right — along with air, water, food and shelter — especially considering the very troubled world into which they never asked to enter. Indeed, mindlessly minding our own business on such matters has too often proven humanly devastating.
But due to the Only If It’s In My Own Back Yard mindset, the prevailing collective attitude, however implicit or subconscious, basically follows: ‘Why should I care — my kids are alright?’ or ‘What is in it for me, the taxpayer, if I support programs for other people’s troubled families?’ While some may justify it as a normal thus moral human evolutionary function, the self-serving OIIIMOBY can debilitate social progress, even when social progress is most needed; and it seems that distinct form of societal penny wisdom but pound foolishness is a very unfortunate human characteristic that’s likely with us to stay.
LikeLike